Platform · Configuration
Your hospital owns the chart.
The longest-running conversation in any hospital-system decision is about change: who changes the chart, when, and at what cost. zMed's answer — your clinical leadership does, the same day, with every change audit-logged and reversible.
Three substrates
zForms · zRules · zFlows
This is what makes zMed work for a 1,200-bed tertiary hospital and a 60-bed secondary hospital on the same software: the configuration moves; the platform does not.
zForms
Every form, owned by the team that uses it
Forms, checklists, consents, assessments and notes — authored and revised in place by clinical and operational teams. Revision-tracked, role-scoped, rolled out per unit, deployable in hours. No software release required for clinical-content changes.
zRules
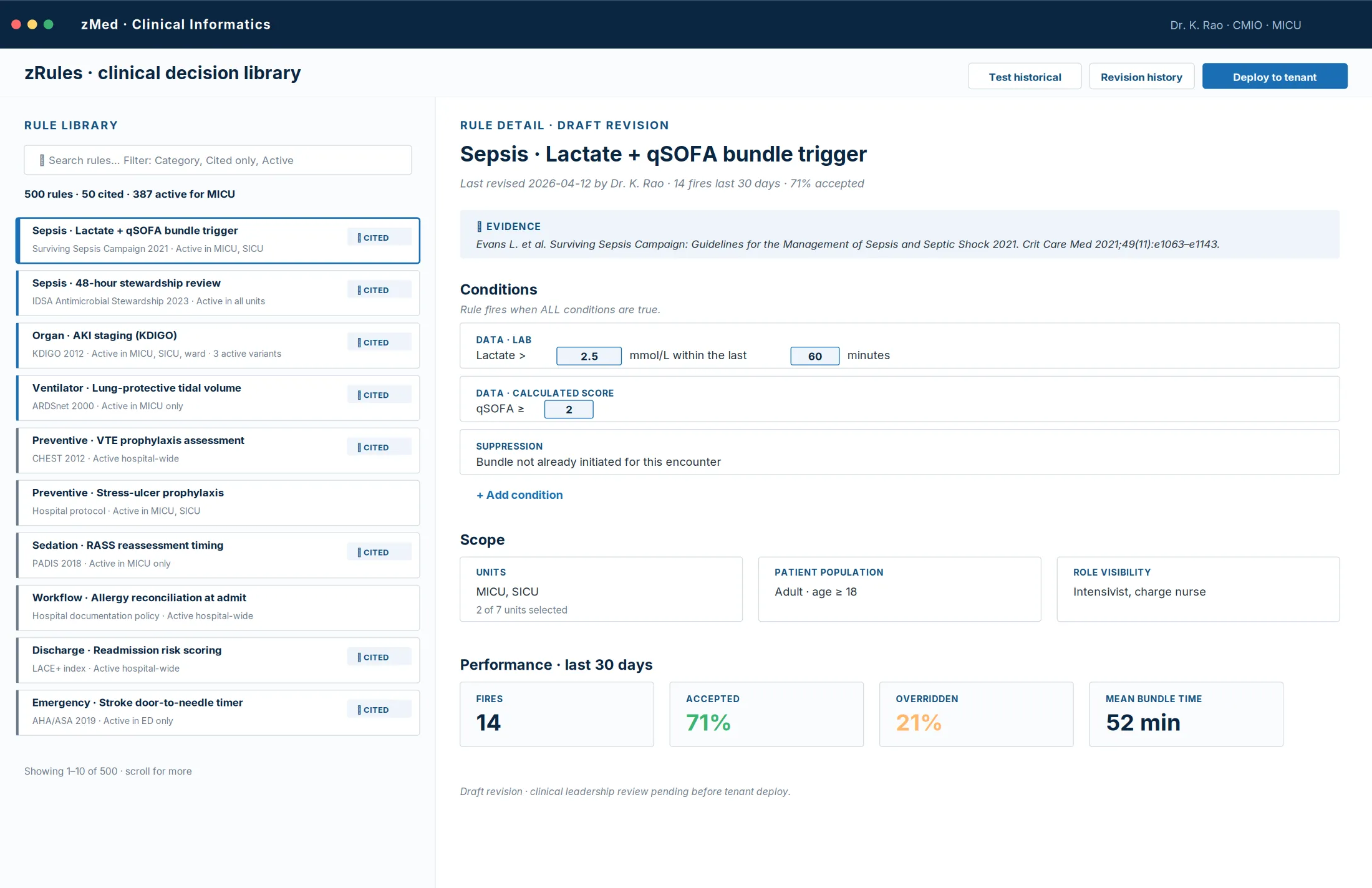
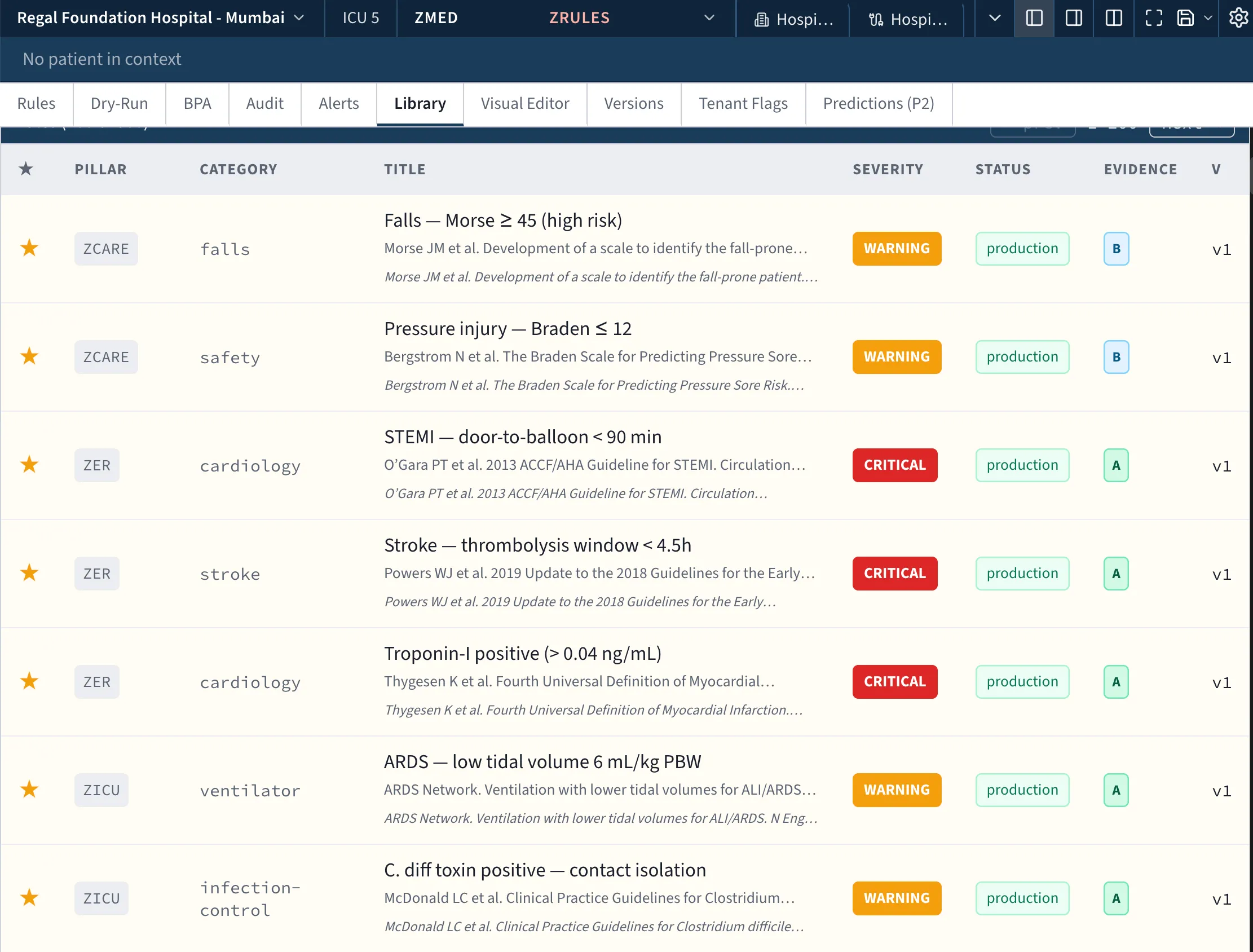
Every rule, with a visual editor
Alerts, scores, suggestions and escalations. Clinical leadership drags conditions onto a canvas, sets thresholds, attaches citations, tests against recent historical data, and deploys per unit — with full revision history and one-click rollback.
zFlows
Every workflow, to your protocol
Admission, rounds, handover, peri-operative checklists, claims — steps, roles, routing, escalations and SLAs defined to the hospital's protocol and changed as practice evolves. Multiple zForms compose into a complete unit workflow.
A worked example
Monday's protocol change, live by Monday afternoon.
Your stroke pathway should include a last-known-well time field, with an alert if that time is more than 270 minutes before arrival. In zMed, the clinical informatics lead opens the stroke pathway form in the visual editor, adds the field, ties it to a rule with a 270-minute threshold, and saves the new revision.
- 01 Rollout scoped to the emergency department only — other units unaffected.
- 02 Every revision captures author, timestamp, rationale and a diff.
- 03 If it causes a problem, rollback is one click — and stays queryable in the audit log.
Governance
Every change tracked. Every author named. Every revision reversible.
Configuration changes land in the same audit log as clinical activity. The quality committee can answer both questions that matter: did the rule fire when it should have — and did it fail to fire when it should have. Overrides carry structured reasons, and the effectiveness dashboard surfaces the rules whose thresholds need revision.
The platform provides the building blocks; the hospital builds the building.
See a configuration change, live
We'll walk through a real form, rule and workflow change in front of your clinical leadership.