Clinical Decision Support (Comprehensive)
Guidance where the decision is made
500 hospital-owned rules — 50 literature-cited — surfaced inline at the moment of decision, with every accept, override and defer logged.
~500
rules in the library at go-live
~50
literature-cited, evidence shown at suggestion
100%
of fires, accepts, overrides and defers logged
What you get
Built for the unit, used by the clinician
- 500-rule library, 50 cited
- Inline, in-chart suggestions
- Accept / override / defer, logged
- Hospital-owned visual editor
Overview
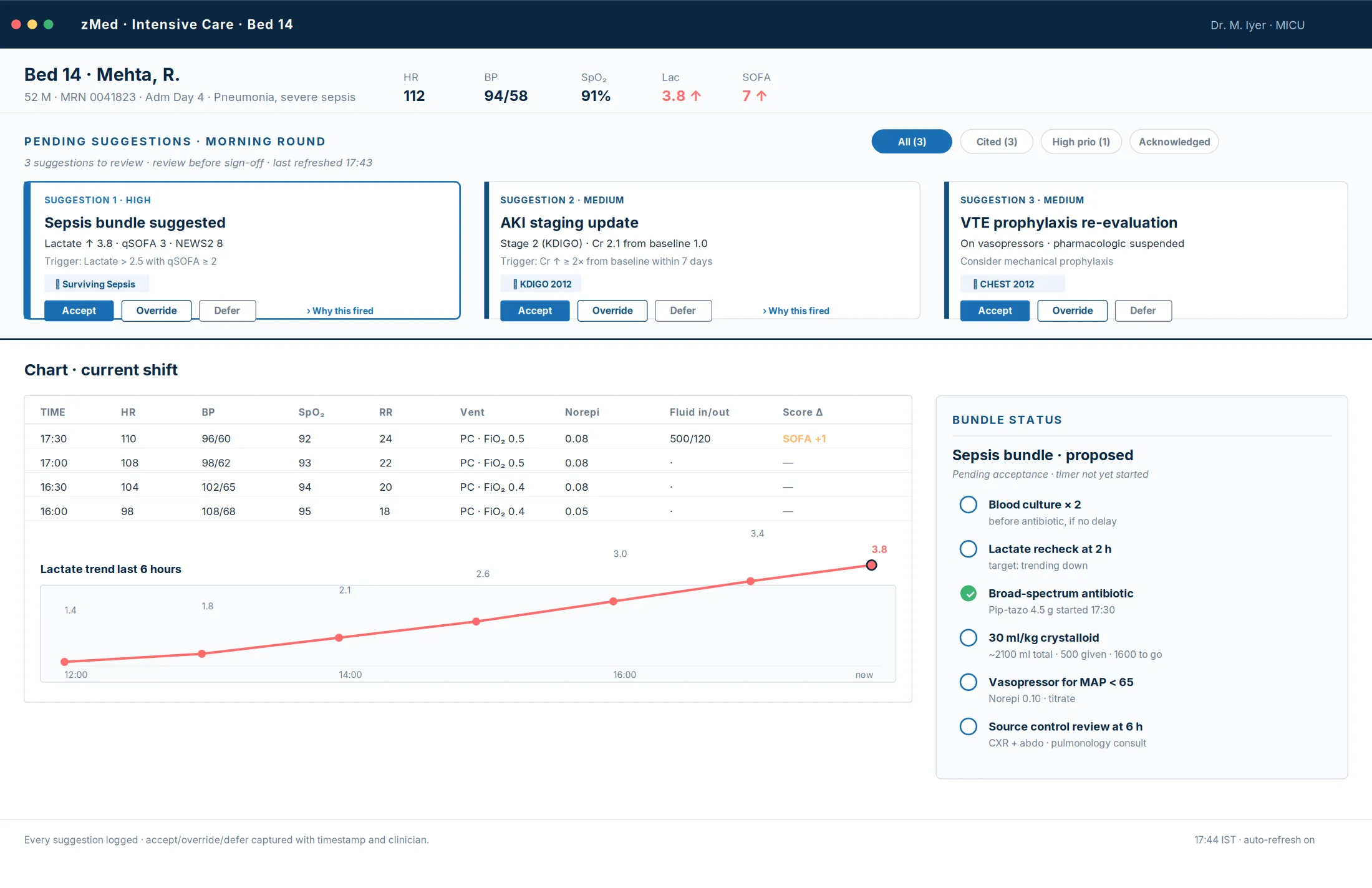
The number of decisions inside a twelve-hour clinical shift is staggering — a dose, an extubation, an antibiotic switch, a fluid bolus, a vasopressor titration. The data is plentiful but unevenly accessible; less than five percent of it is read before the next clinical decision. Traditional decision support delivered through a separate portal or an hourly summary email does not survive the cadence of the unit: by the time the clinician opens the tab, the moment of decision has passed. zMed's answer is to put the suggestion where the decision is made.
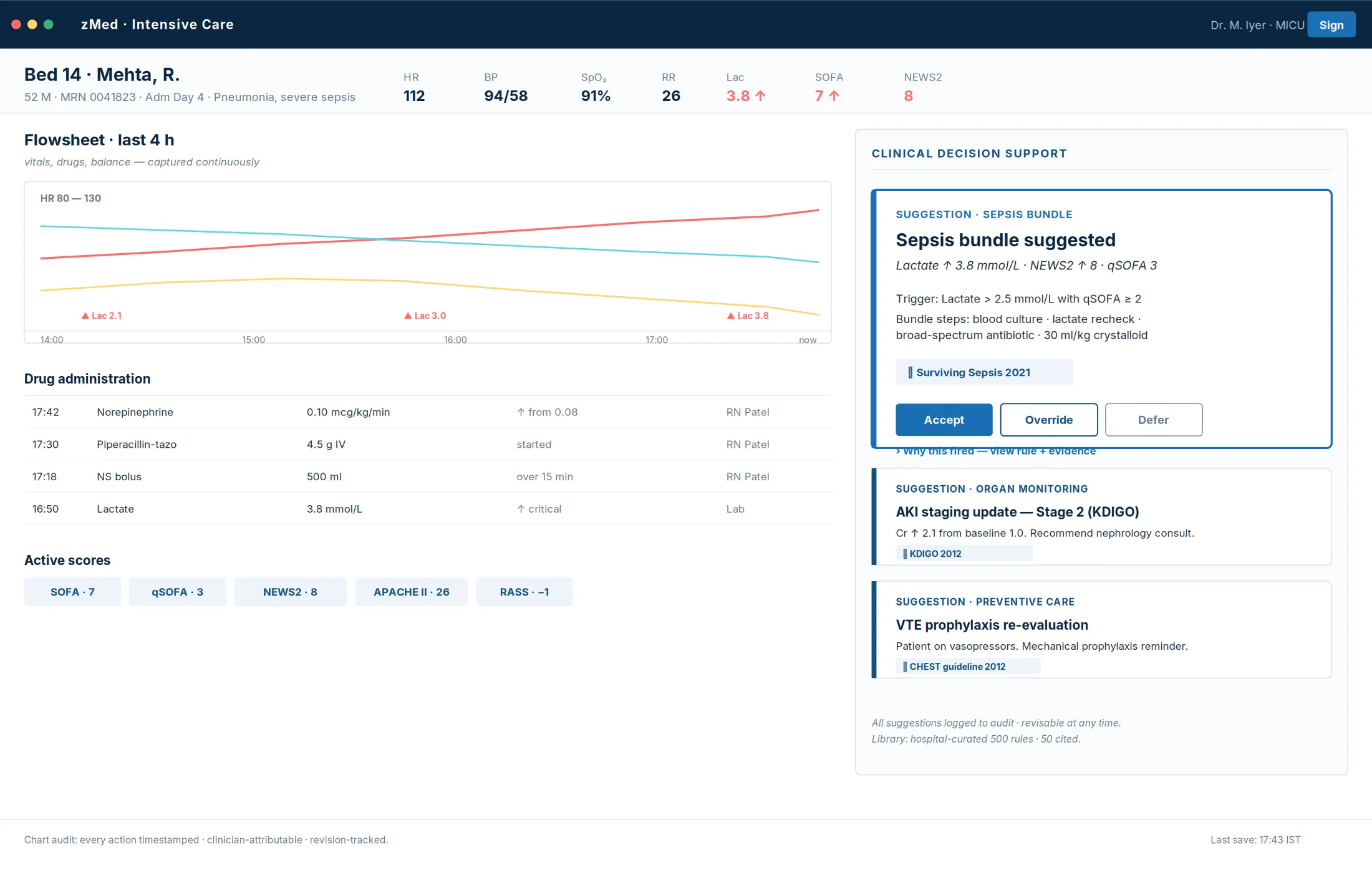
The rule engine runs continuously, against every patient, in every unit, without the clinician asking for it. It subscribes to the chart's event stream, and when a relevant event arrives it evaluates every rule whose trigger includes that event, with the patient's current context attached. The result surfaces inline — a native flowsheet row, an order-set prompt, a medication sign-off card — and every evaluation is logged whether it fires or not, answering both questions the quality committee asks: did the rule fire when it should have, and did it fail to fire when it should have.
The most important property is ownership. The visual editor lets clinical leadership drag conditions onto a canvas, set thresholds, attach citations, test a new rule against recent historical data, and deploy it per unit — all without engineering involvement and without waiting for a vendor release cycle. Every revision captures the author, the timestamp, the rationale and a diff; every retired rule stays queryable in the audit log.
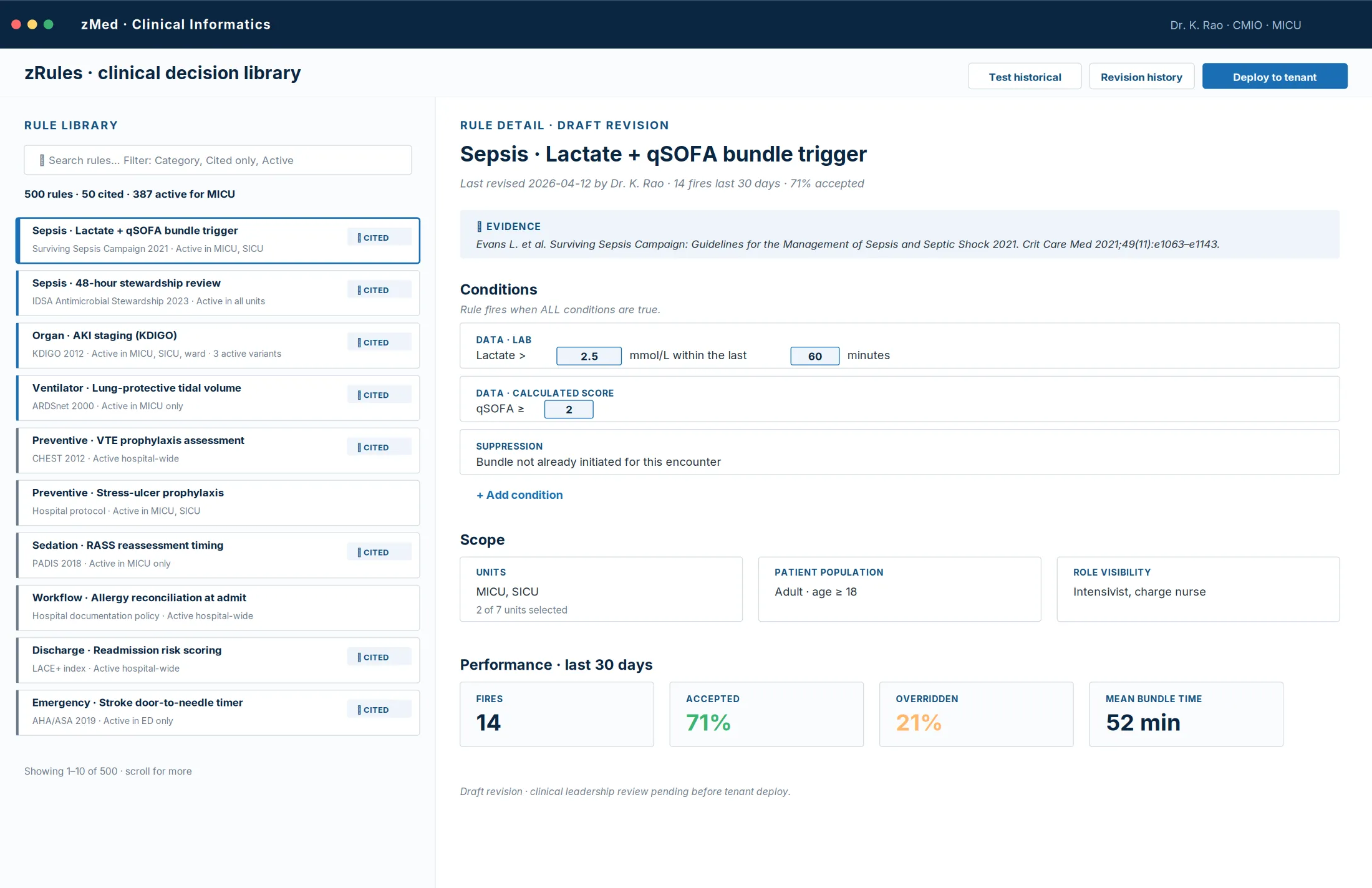
The rule library
- ~500 rules at go-live, ~50 literature-cited
- Sepsis bundles, drug–drug and drug–allergy interactions, renal dose adjustment, VTE prophylaxis, early-warning escalation, and the bundle state machines for the operating room, emergency and ward. Citations surface at the moment of suggestion, so the clinician reads the evidence, not just the flag.
- Hospital-authored growth
- Over the first year a typical library grows well beyond the foundation — rules added, revised and retired continually by the hospital, every change versioned.
Automated clinical scores
Twelve foundational scores recalculate continuously as data arrives, each value carrying its literature citation. The same engine activates additional scores at go-live and supports hospital-authored scores throughout.
- The foundational twelve
- SOFA, qSOFA, APACHE II, NEWS2, CAM-ICU, KDIGO AKI staging, ARDS severity (Berlin), shock-type classification, SAT/SBT readiness, VTE adherence, glycemic tier, and pressure-injury risk — recalculated the moment the chart holds new data, never on a schedule.
- Cited, not claimed
- Every score value shows the calculation basis and the citation behind it. The audit reviewer sees the evidence alongside the number.
Care bundles as state machines
- Sepsis bundle, timed end to end
- The 1-hour, 3-hour and 6-hour bundle lights up the moment the chief complaint is named, tracks every element — lactate, cultures, antibiotics, fluids — and times each step against the protocol.
- Pathway machines across units
- Stroke, trauma, chest pain and peri-operative bundles run as the same state machines in the ED, OR and ward — adherence visible live, every deviation logged for the quality review.
Smart alarm management
Alarm fatigue is the largest single source of clinician burnout in the ICU. zMed cuts alarm load 60–85% — at three levels.
- At the source
- Waveform-derived lethal alerts carry self-cooldown; cycle anomalies (a cuff reading the floor of its range three times) prompt a re-cuff instead of three sequential alarms.
- At the corroboration layer
- Single-observation alerts are downgraded; alerts where two or more modalities agree are escalated. A corroboration score gates severity.
- At the override-pattern layer
- Every override is captured with a structured reason. A rule that fires often without acceptance reveals itself on the effectiveness dashboard — a noisy rule is a tunable rule, and a tunable rule is a hospital-owned rule.
Numeric analytics — the quiet trends
- Trend computation
- First and second derivatives of vitals over rolling windows. The slow drifts that never fire an isolated alarm are exactly what feeds the early-warning rules — and the predictive models in Clinical AI.
- Cross-modal corroboration
- An SpO₂ drop is upgraded when the plethysmograph confirms it and downgraded on obvious motion artefact; a blood-pressure spike is verified against the arterial trace when one is present.
- False-alarm scoring
- Every alert candidate carries a computed false-alarm likelihood. High-likelihood artefacts are gated — and the suppression itself is logged.
Audit & effectiveness
- Every interaction logged
- Fire, surface, acknowledge, resolve, override, escalate — the alert lifecycle is consistent and auditable end to end, with clinician identity at every step.
- The override is the feedback
- Override reasons are the system's primary improvement signal: rules dominated by "not clinically relevant" surface monthly to clinical informatics as retuning candidates. The closed loop runs from chart event to the next quarter's rule revisions.
The platform supports the clinician; the clinician decides; the audit log captures every decision. The machine-learning layer that works alongside these rules — the predictive risk models, real-time waveform analytics and AI drafting — is covered under Clinical AI.
Explore more
Other modules & products
ICU & Critical Care
Every bedside signal, read every minute
Tele-ICU & Command Center
One specialist, every bed, every site
Operating Room & Anaesthesia
The chart that writes itself
Emergency & Triage (ER)
The pathway opens at the door
Ambulance & Pre-Hospital
Care that starts before arrival
HIS & ERP
One platform, not two systems
Clinical AI (Comprehensive)
“Is this about to happen?”