Emergency & Triage (ER)
The pathway opens at the door
Acuity and vitals at registration, the right pathway tab opening at the chief complaint, and disposition in a single action.
5-level
acuity triage at the door
Minutes
door-to-bundle, timed end to end
1 action
disposition — admit, transfer, observe or discharge
What you get
Built for the unit, used by the clinician
- Five-level acuity triage
- Self-opening pathway tabs
- Door-to-bundle timers
- One-action disposition
Overview
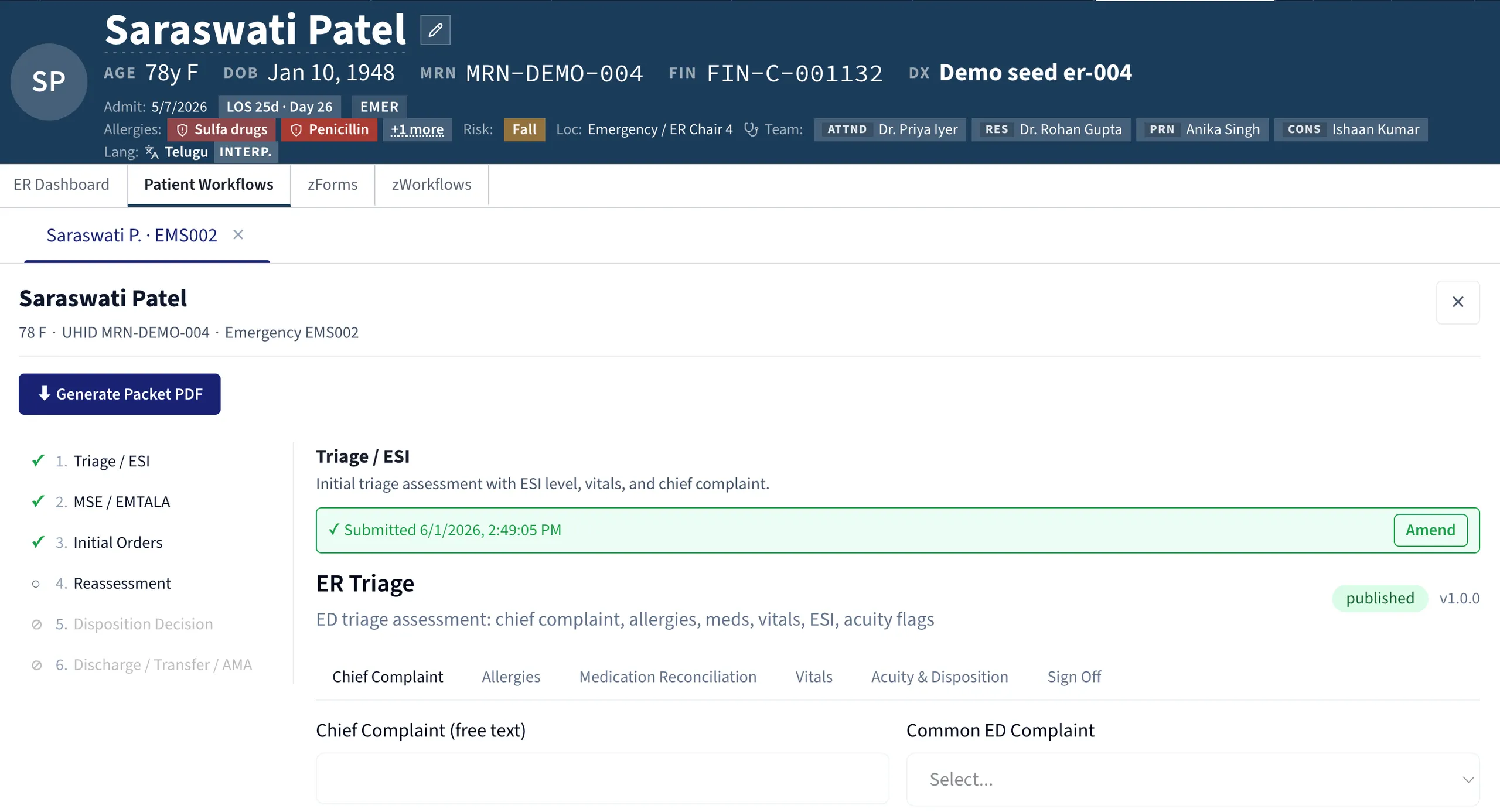
The emergency department is not a unit so much as a transit hall. A patient arrives, is triaged, is worked up, is decided, is dispositioned, and is gone — and a thousand more will follow the same path. The system that runs the department has to be one screen for every clinician, every shift, every minute, with throughput that matches the door. zMed is built for that cadence: the chart opens at triage, the workflow tabs open at the chief complaint, and the disposition opens at the decision, each step taking seconds rather than minutes.
Triage is the first and most leveraged decision. A five-level acuity scale, a structured chief complaint drawn from a hospital-configured list, and a full set of vitals — heart rate, blood pressure, SpO₂, temperature and respiratory rate — are captured by the triage nurse at the door. Bay assignment follows from acuity, and the first observation interval follows from the bay. The chart starts before the patient sits down, and the chief complaint sets the pathway in motion.
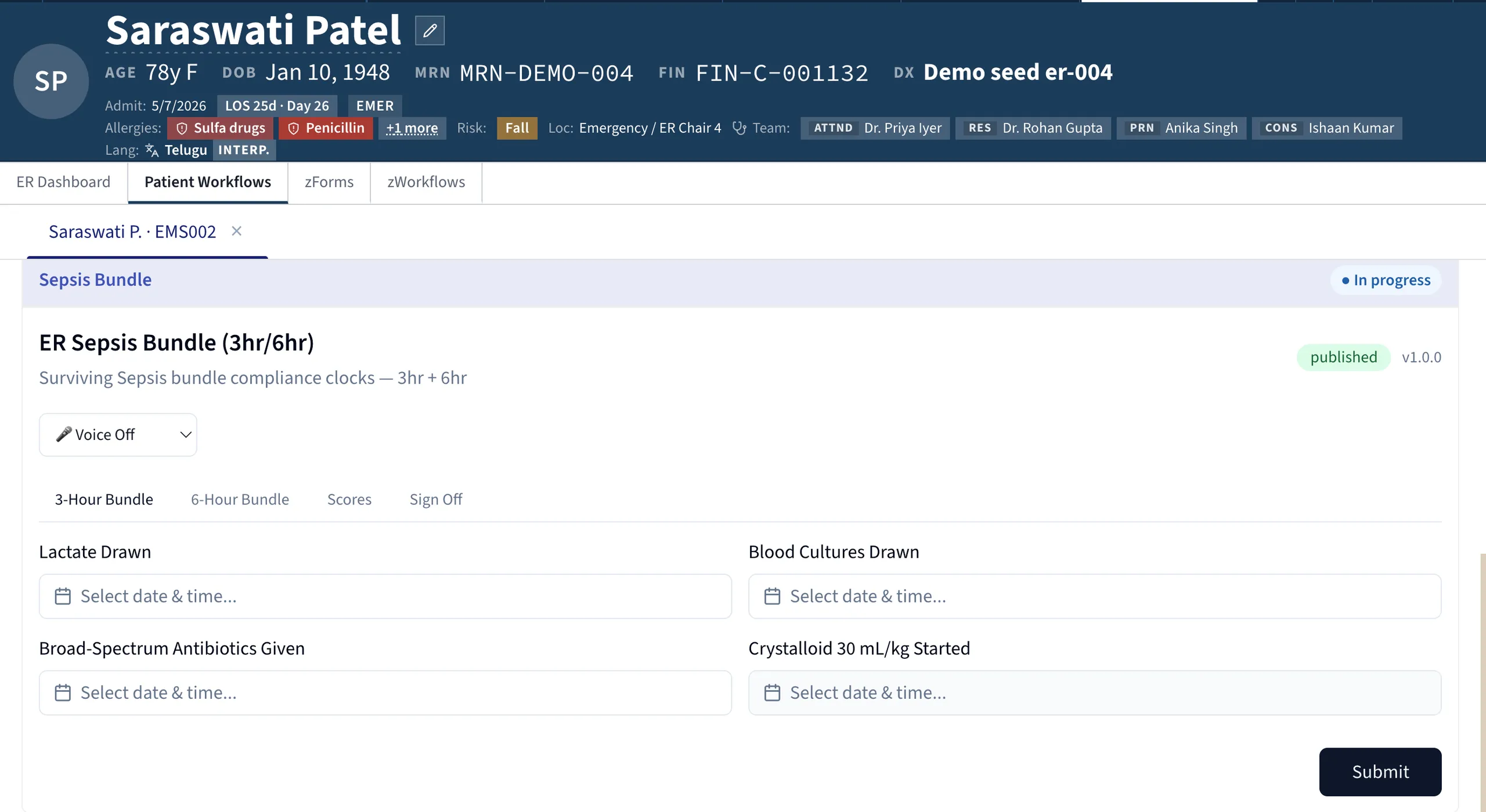
That is where the workflow tabs earn their place. A patient click does not open a generic chart and ask the clinician to choose; it opens the chart with the right pathway already in front, the defaults already loaded, and the timer already running. A suspected sepsis case opens a bundle checklist — lactate, blood culture, broad-spectrum antibiotic, fluid bolus — with a door-to-bundle timer counting. Chest pain primes the ECG and troponin order; a stroke alert starts the door-to-needle clock; a trauma activation opens the bay with role allocation visible. The result is that the sepsis bundle starts at minute twelve rather than hour two, and the trauma activation fires before the team arrives rather than when the surgeon walks in. Every pathway is owned by the hospital: clinical leadership extends the library, edits a default, or scopes a pathway to a specific shift, with changes deploying in hours and every run, step and override kept for the quality review.
Medico-legal cases carry documentation requirements the rest of the chart does not, and the MLC sub-workflow handles them in line with the clinical record — structured incident documentation of time, place, parties and injuries; dated photographs attached with a per-photograph chain-of-custody audit row; and police notification logged with timestamp and officer.
Finally, disposition — admit, transfer, observe or discharge — is the second-most consequential moment in the stay, and zMed makes it a single action. The selection opens the destination workflow, the handoff summary drafts itself from the structured chart for the clinician to edit and sign, and the receiving unit is notified the instant the disposition is recorded. Door-to-disposition is timed end to end, and the department's KPIs — length of stay by disposition, left-without-being-seen, return-within-72-hours — surface from the same record, audit-ready.
Explore more
Other modules & products
ICU & Critical Care
Every bedside signal, read every minute
Tele-ICU & Command Center
One specialist, every bed, every site
Operating Room & Anaesthesia
The chart that writes itself
Ambulance & Pre-Hospital
Care that starts before arrival
HIS & ERP
One platform, not two systems
Clinical Decision Support (Comprehensive)
Guidance where the decision is made
Clinical AI (Comprehensive)
“Is this about to happen?”