Operating Room & Anaesthesia
The chart that writes itself
The whole peri-operative journey on one record — auto-captured anaesthesia charting, enforced surgical safety, and notes that draft themselves.

~140
chartable fields per case — device-sourced majority auto-captured
3
safety moments: sign-in, time-out, sign-out
0
retyping — case documents draft themselves
What you get
Built for the unit, used by the clinician
- Auto anaesthesia record
- Surgical safety checklist
- Live theatre worklist
- Self-drafting summaries
Overview
The operating room is not the ICU. The cadence is different, the documentation is different, and the audit is different. Anaesthetists chart minute by minute; surgeons document in the moments between procedures; theatre coordinators run the list at a level above any single case. zMed's operating-room module is built for the cadence of the room while staying connected to the rest of the platform for the journey before and after, so all three roles work from one record without being forced into one workflow.
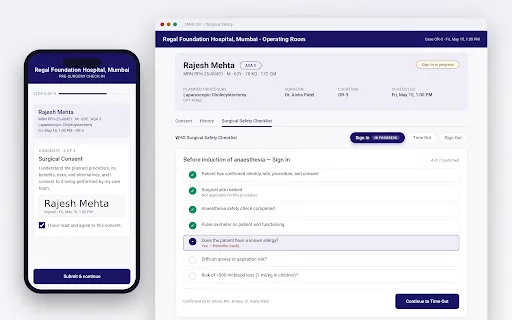
It begins before the room is ready. Pre-operative check-in runs on a tablet at the patient-holding area, capturing digital consent with signature and date, a confirmed health summary of allergies, prior surgeries and comorbidities, and the surgical safety checklist run as three distinct moments — sign-in, time-out and sign-out — each recorded with the team that performed it. The operating room receives a prepared patient, not a problem, and the morning briefing happens against a real, complete chart rather than a hand-typed summary from the night before.
Intra-operatively, the anaesthesia flowsheet is the working surface. Continuous trend curves for heart rate, blood pressure, SpO₂ and EtCO₂ sit at the top of the screen, captured automatically at the cadence the monitor produces. The drug log sits immediately below — every drug, every dose, every time, totalled across the case and queryable across the unit. Event markers run along the time axis, each one a single tap. The anaesthetist charts by exception rather than by re-entry, which means attention stays on the patient. A typical adult general-anaesthetic case carries around 140 chart-able fields; the device-sourced majority is captured automatically, leaving a single clear prompt for the handful only a clinician can supply.
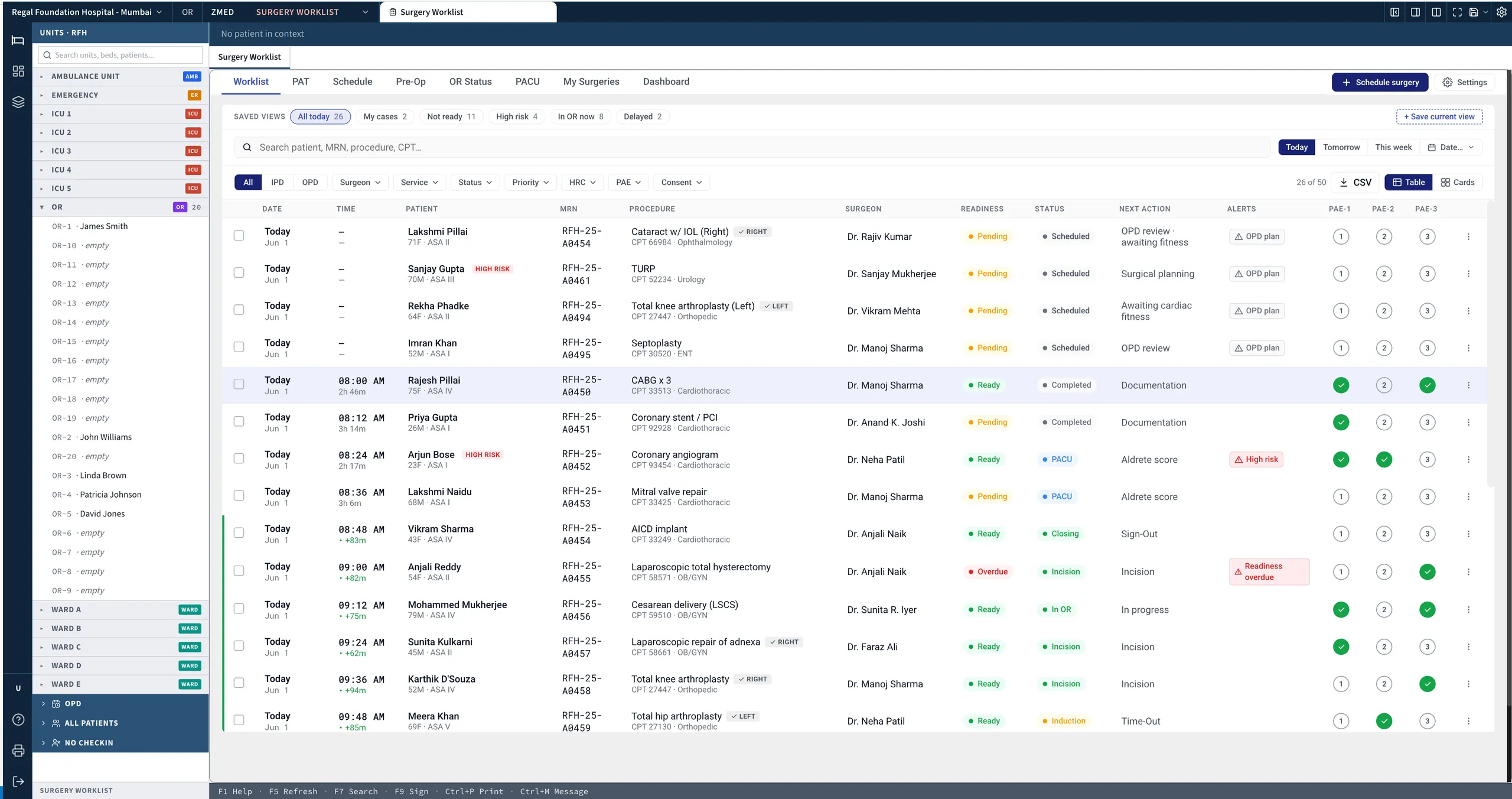
Above the individual case, the surgery list gives theatre coordinators a live grid of every case in every theatre — awaiting, in progress, recovery — with surgeon and team allocation visible at a glance and delay reasons captured at the moment they occur, ready for the morning review.
When the case ends, the documents draft themselves. The operative note builds from the surgical event timeline, the anaesthesia summary from the flowsheet and drug log, and the recovery handoff from the last twenty minutes of vitals. Each is edited as needed, signed in the chart and dispatched to the receiving unit before the patient leaves the table — so the operative record is closed before the recovery bay, and every case flows end to end from chart to report with no retyping.
Explore more
Other modules & products
ICU & Critical Care
Every bedside signal, read every minute
Tele-ICU & Command Center
One specialist, every bed, every site
Emergency & Triage (ER)
The pathway opens at the door
Ambulance & Pre-Hospital
Care that starts before arrival
HIS & ERP
One platform, not two systems
Clinical Decision Support (Comprehensive)
Guidance where the decision is made
Clinical AI (Comprehensive)
“Is this about to happen?”