Tele-ICU & Command Center
One specialist, every bed, every site
A single command centre watching every critical bed across many hospitals — same chart, same scores, same orders as the bedside.
1
command grid across every covered site
4–6h
sepsis surfaced pre-clinical, network-wide
60–85%
alarm load suppressed at scale
What you get
Built for the unit, used by the clinician
- Multi-site command grid
- Two-way remote intervention
- Early-warning at scale
- One network-wide audit log
Overview
Tele-ICU answers a structural shortage. Intensivists are scarce, and many hospitals — particularly smaller and regional sites — cannot staff round-the-clock critical-care expertise at every bed. zMed's tele-ICU configuration extends one unit's intensivist coverage across an entire network of hospitals, and it does so without creating a second system to learn, license or reconcile. The defining property is sameness: the remote command centre runs the same chart, the same scores, the same alerts and the same intervention workflows as the bedside.
The central command grid is the working surface. Every covered patient across every covered hospital appears in one view, with each tile carrying the patient's key vitals, latest score and acuity colour. The remote intensivist filters by acuity to triage the sickest first, by hospital to focus a single site, or by alert state to clear active warnings. From across a network the scarcest specialist watches the widest population of risk, and the grid keeps that population legible at a glance rather than scattered across separate logins.
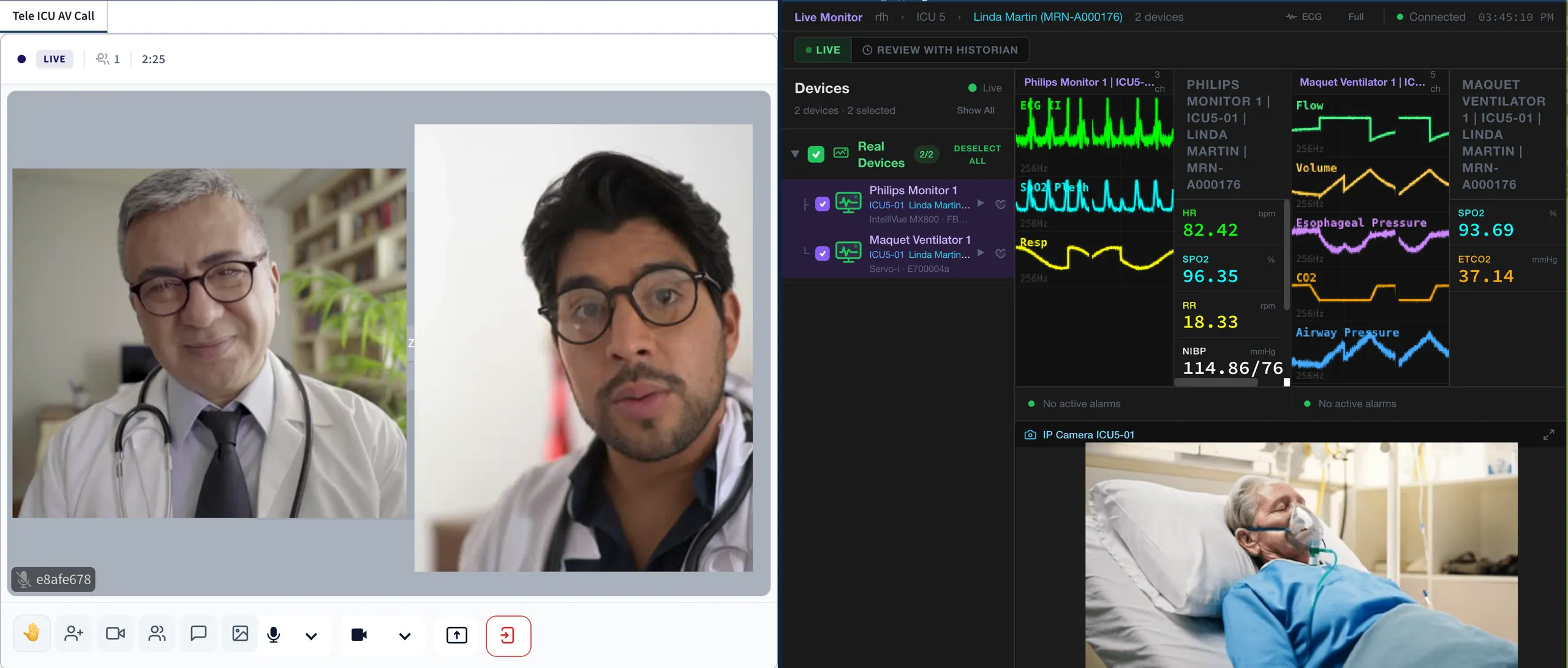
The hub-and-spoke connection is the platform itself, not an interface project. The hub hospital runs the command centre; each spoke hospital's zMed deployment — cloud, on-premises or edge-appliance — streams its covered beds to the hub over a secure link, so the spoke's bedside chart and the hub's grid are the same record with no synchronisation layer in between. Bedside device data, scores and alerts arrive at the hub at the same cadence the spoke's own nurses see; IP-camera views bring the bedside into the command centre; and built-in audio-video collaboration connects the hub intensivist with the spoke's bedside team in one tap, documented in the same chart. A spoke can join the network in days — it is enrolment, not integration — and if the link drops, the spoke continues charting locally and reconciles when connectivity returns.
Underneath each tile is the full continuous chart. Twelve clinical scores recalculate continuously from the same flowsheet feed the bedside generates, each carrying its literature citation. Predictive intelligence surfaces deterioration and sepsis 4–6 hours pre-clinical, and smart suppression keeps alarm load down 60–85% so the centre responds to genuine signal rather than alarm fatigue multiplied across many beds. Every piece of this intelligence is advisory only; clinical judgement always wins, and each suggestion is logged with accept, override or defer plus the reason.
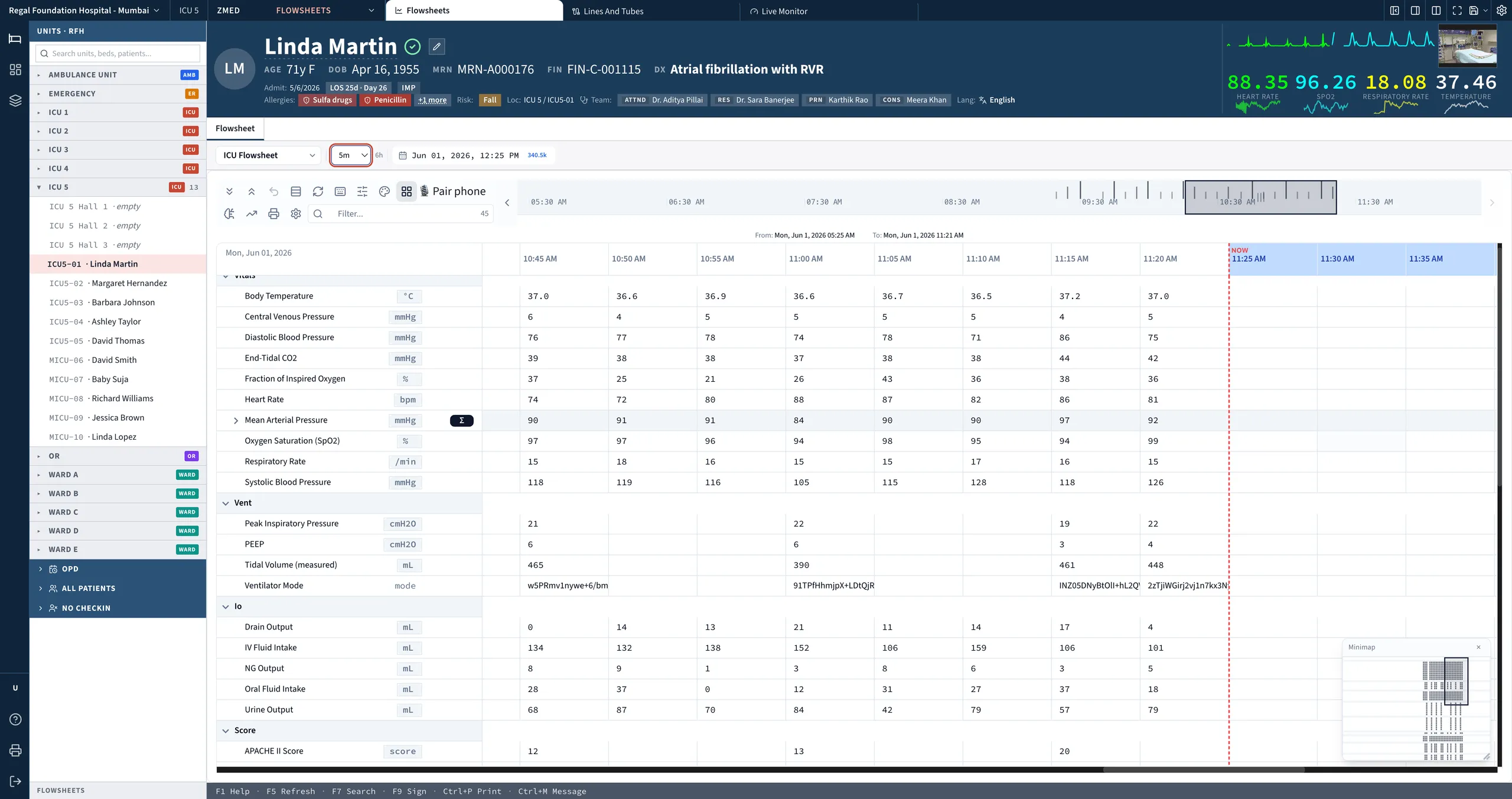
Intervention is two-way and real. The remote intensivist can open a patient's chart from the alert, fire orders, sign the chart and document the consult inline — without a phone call to the bedside. Because the remote and bedside clinicians work from one document, handoff is seamless: nothing is re-keyed, nothing is reconstructed from a phone conversation, and the timeline reads as one continuous record regardless of who acted or where they sat.
Governance follows the same one-record principle. A single audit log spans every site in the network, so compliance reporting, override traceability and quality surveillance operate for the whole network rather than hospital by hospital. Standard dashboards roll up census, throughput and bundle compliance across the covered sites. For a hospital group, that means one platform and one audit trail covering remote coverage and bedside care together — reach extended across many sites, with the record kept whole.
Explore more
Other modules & products
ICU & Critical Care
Every bedside signal, read every minute
Operating Room & Anaesthesia
The chart that writes itself
Emergency & Triage (ER)
The pathway opens at the door
Ambulance & Pre-Hospital
Care that starts before arrival
HIS & ERP
One platform, not two systems
Clinical Decision Support (Comprehensive)
Guidance where the decision is made
Clinical AI (Comprehensive)
“Is this about to happen?”