Emergency & pre-hospital network · West India · Metropolis · One metropolis · ambulance fleet to ER on a single record
The ER that knows the patient before the doors open
Anonymized deployment · reference conversations arranged for qualified evaluations
Before arrival
patient vitals visible to the ER team
Minutes
door-to-triage, measured on every case
100%
medico-legal cases with complete statutory documentation
Weeks
from kickoff to first live ambulance
An emergency and pre-hospital network in a West Indian metropolis runs its ambulance fleet and emergency department on one record: the enquiry call becomes a tracked dispatch, the crew’s chart travels ahead of the vehicle, and the ER receives a patient it already knows.
The challenge
In a large metropolis, the gap between an emergency call and definitive care is paved with phone calls. The enquiry desk took calls on one system — or on paper. The dispatcher chose a vehicle without seeing where the fleet actually was. The crew radioed ahead if the line held, and the ER met the patient at the door knowing little more than a one-line summary. Vitals taken in the vehicle were taken again from scratch at triage, and the minutes between the door and first clinical contact were nobody’s number — unmeasured, so unmanaged.
Medico-legal cases — a substantial share of any metropolitan emergency workload — carried a further burden: statutory documentation depended on individual diligence under pressure, with gaps discovered only when the records were demanded later.
The deployment
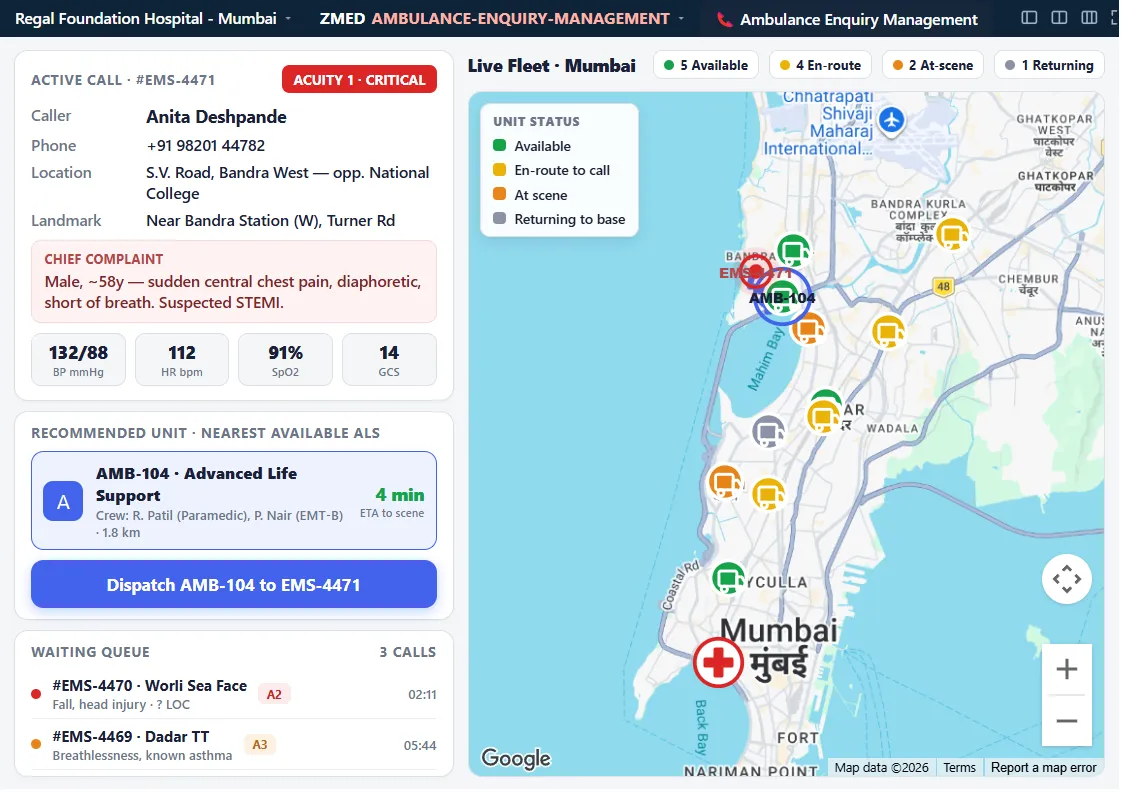
The network put the whole pre-hospital pathway on one record. An enquiry call becomes a dispatch on a single screen: the desk captures the caller’s details once, the dispatcher sees every vehicle live on the map and assigns the nearest appropriate ambulance, and the job — with its timings — is part of the record from the first ring.
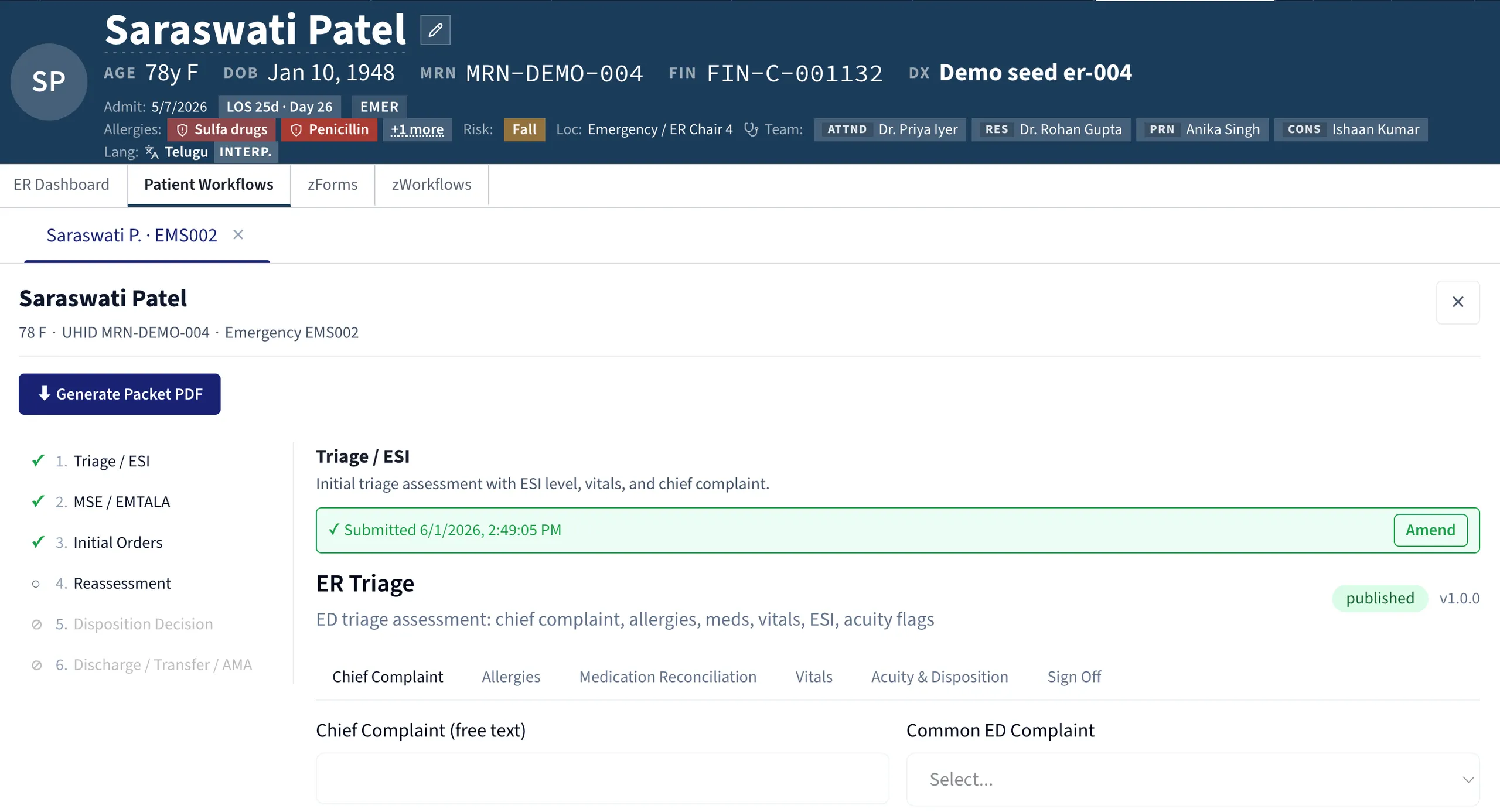
En route, the crew charts into the same record the hospital uses. That is the chart-ahead handoff: the vitals, interventions and trend recorded in the vehicle are visible to the ER team before arrival, so the receiving team watches the patient approach on the map and prepares the bay to match what the numbers show — not to a guess.
At the door, triage runs with acuity banding, and door-to-care clocks start automatically on every case, so the department manages its minutes rather than estimating them. For medico-legal cases, the statutory workflow is built into the chart itself: the required documentation is completed as care proceeds, not reconstructed from memory after the shift.
The first ambulance went live within weeks of kickoff, and the fleet followed vehicle by vehicle — each crew trained on its own vehicle, on real runs.
What changed
Patient vitals visible to the ER before arrival. The handover begins before the doors open. The receiving team confirms what it has already read, instead of hearing it for the first time in the corridor.
Door-to-triage measured in minutes, on every case. Not sampled, not audited retrospectively — clocked automatically on every arrival, so the department can see its own performance shift by shift and act on it.
100% of medico-legal cases with complete statutory documentation. Because the workflow is part of the record rather than a parallel form, completeness stopped depending on how busy the night was.
Weeks from kickoff to first live ambulance. The network proved the pathway on one vehicle and one department, then scaled — no long programme standing between decision and benefit.
What the team says
The head of emergency medicine for the network describes the change at the door:
“We used to meet the patient at the door and start from zero. Now the team has read the vitals, seen the trend and prepared the bay before the ambulance turns into the gate.”
Starting from zero is the old default of pre-hospital care: whatever happened in the field arrived as a verbal summary, compressed and perishable. What the team values most is not any single screen but the removal of that reset — the patient’s story now arrives intact, ahead of the patient, and the first minutes in the department are spent treating rather than re-asking.
“We used to meet the patient at the door and start from zero. Now the team has read the vitals, seen the trend and prepared the bay before the ambulance turns into the gate.”
Head of Emergency Medicine, metropolitan acute-care network
Every figure above is measured as described on the methodology page. Thinking about replacing an incumbent system? Here is how the seam is managed.